Ulcerative Colitis:
Inflammation and ulcers restricted to colon and rectum
Sypmtoms
- Diarrhoea (may contain pus or mucus)
- Abdominal pain
- Some may experience flare up and these symptoms include:
-Painful and swollen joints (arthritis
mouth ulcers
-Swollen fat under the skin causing bumps and patches – this is known as erythema nodosum
-Irritated and red eyes
-Weight-loss
-Fatigue
-Problems with bones, such as osteoporosis
Diarrhoea associated with ulcerative colitis is sometimes treated with anti-diarrhoeal drugs (such as loperamide hydrochloride or codeine phosphate) on the advice of a specialist
Contraindicated in acute UC flare ups: Loperamide hydrochloride and codeine phosphate as this increases the risk of toxic megacolon.
Longterm Problems
- An increased risk of developing bowel cancer
- Poor growth and development in children and young people
- Osteoporosis- because of using steroid medicines treat ulcerative colitis
- Toxic megacolon
- Venous Thromboembolism
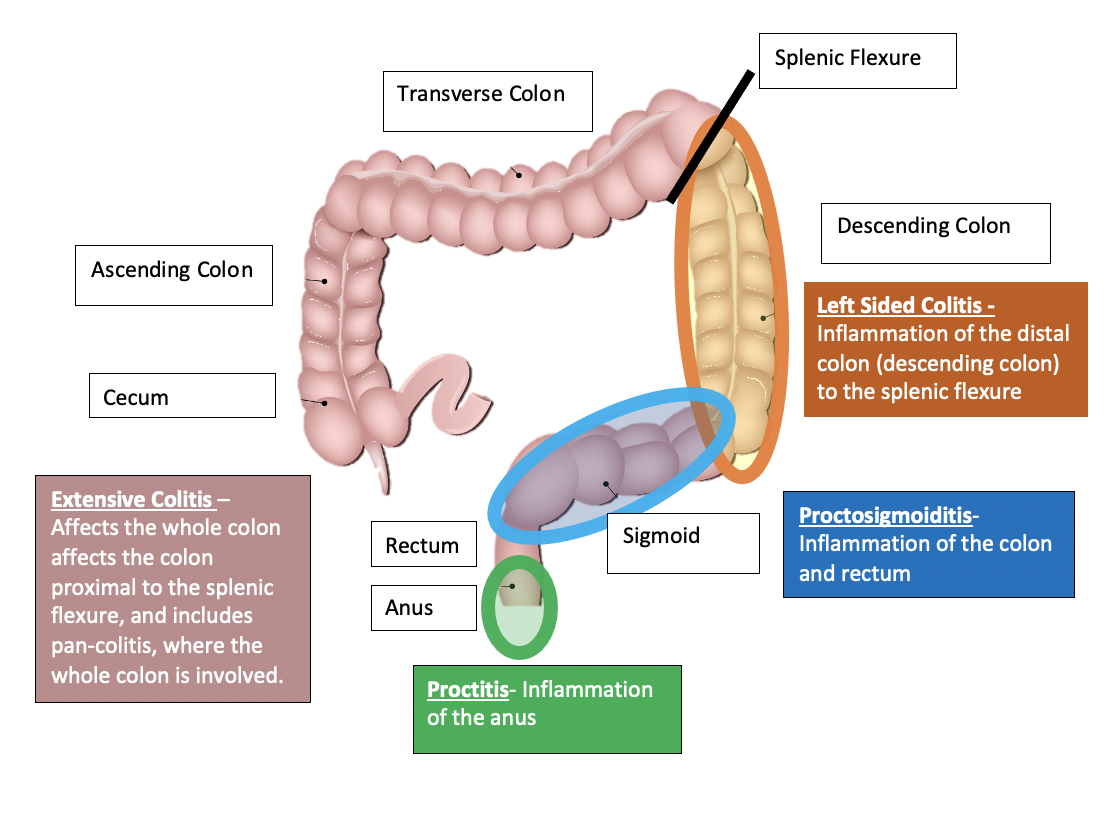
Treatment is based on the severity and which part of the colon is affected